Opt-Out Organ Donation for the U.K.?
The BBC reports that a change may be in the offing in Britain’s policies on cadaveric organ donation:
Gordon Brown says he wants a national debate on whether to change the system of organ donation. He believes thousands of lives would be saved if everyone was automatically placed on the donor register. It would mean that, unless people opted out of the register or family members objected, hospitals would be allowed to use their organs for transplants. But some critics say the state should not automatically decide what happens to people’s bodies after they die. Currently there are more than 8,000 people waiting for organ transplants in the UK - a figure which rises by about 8% a year. Writing in the Sunday Telegraph newspaper, the prime minister said a system of “presumed consent” could make a huge difference. … The system already operates in several other European countries and has boosted the number of organs available for transplant.
My view is that Gordon Brown is wrong, but not for the reasons you might think.
The claim that “presumed consent” systems perform better than “informed consent” systems is not well supported empirically. If you look at cadaveric organ procurement rates in the OECD over the past 12 years or so, we find that presumed-consent systems do in fact perform better on average than informed-consent systems. The question is why they do so. Debate in this area is dominated by bioethicists, economists and lawyers. A consequence of this is that—thanks to the disciplinary interests and biases of these groups—the organizational and institutional machinery required to make something as complex as cadaveric donation happen tends to drop away in debates, and is replaced by considerations of the ethical implications of this or that policy in general (e.g., concerning consent) or arguments about the effect of this or that incentive or rule on individuals (e.g., concerning financial incentives or a legal regulation). But the organizations matter because they manage the logistics of procurement, and this is a very complex process. How a change in the law is implemented in practice, or how a rule is embedded in organizational process, can greatly affect the outcomes. This is more a question of organizational and institutional sociology.
Advocates for presumed consent say that most people support donation anyway and it is only a failure to record their wishes, or the meddling intervention of next-of-kin, which prevents that preference from being carried out after their deaths. However, it turns out that most OECD countries with a nominally presumed consent system also allow for a de facto next-of-kin veto on procurement. (The exceptions are Austria and, to a lesser degree, Belgium.) So things are not so straightforward. Nevertheless, presumed consent countries do a bit better on average. The question is, why?
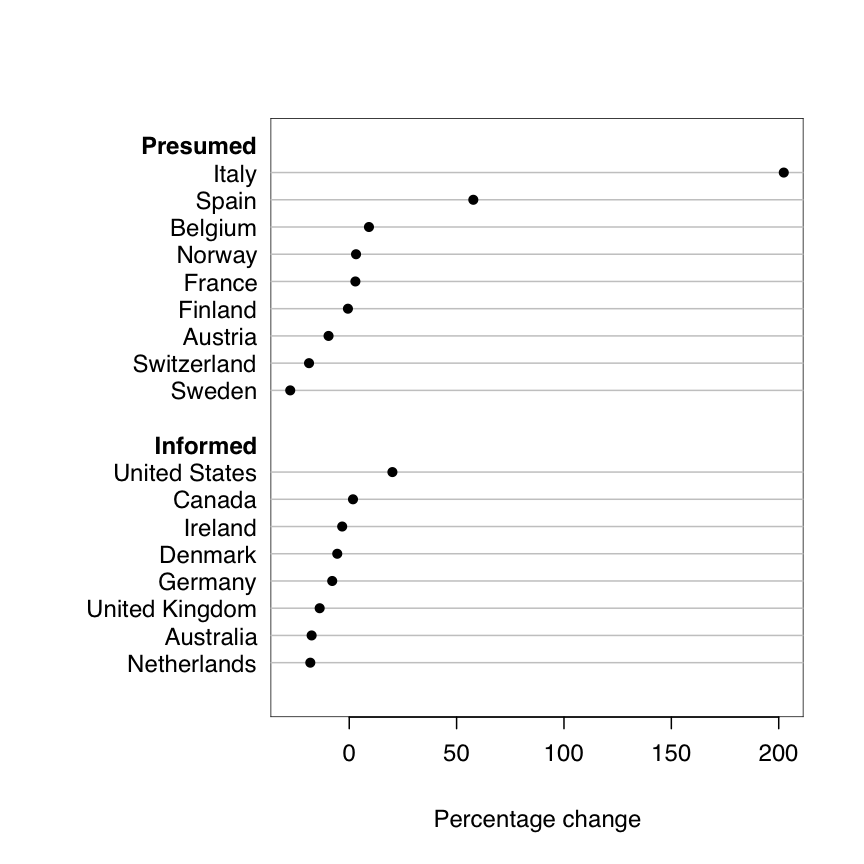
Here’s a chart showing the average increase in the procurement rate for a number of presumed- and informed-consent countries between 1990 and 2002. The dots represent the difference between the average procurement rate between 1990-1994 and 1998-2002. You can see right away that while most countries (regardless their consent rule) showed modest growth between the two time periods, the increase in Spain and (especially) Italy is much larger. These changes were not brought about through changes in the law, but rather through investment in the organizational underpinnings of the procurement system. Reform of the rules governing consent is often accompanied by an overhaul and improvement of the logistical system, and it is this—not the letter of the law—that makes a difference. Cadaveric organ procurement is an intense, time-sensitive and very fluid process that requires a great deal of co-ordination and management. Countries that invest in that layer of the system do better than others, regardless of the rules about presumed and informed consent.
And, indeed, the BBC report notes—in passing!—that the Task Force recommending the switch to presumed consent laws also recommends that twice as many transplant co-ordinators be hired and that specialized 24-hour transplant teams be set up. These are the changes that will really make a difference. I think that the main effect of a change in the law, if it happens, will be as a public signal to prospective donors (and their next of kin) that the socially accepted default option on donation has shifted from “Ask permission” to “You have to object.” But I will be very surprised if medical teams in the UK feel they can disregard the wishes of next-of-kin who strenuously object to organ procurement.
An organizational perspective on the procurement system is less common than you might think. Instead, debate focuses on the ins and outs of hypotheticals about consent, the wishes of individuals, and so on. Discussion threads tend to focus on cases where particular individual cases meet abstract principles of rights or ethics. But in practice this kind of thing doesn’t happen at all without a tremendous amount of organizational work, and most of the variation we observe in cadaveric procurement rates is less a consequence of general legal frameworks and more the result of material differences in the short-run logistical work and long-run cultural effort of procurement organizations.
If you’re interested in this stuff, I make this general argument at greater length (and with more data) in this paper.